Insulin Co-Pay Cap Laws
Co-pay caps are the most recent debate amongst diabetes advocates around the United States: Are they helpful or hurtful to the insulin access movement?
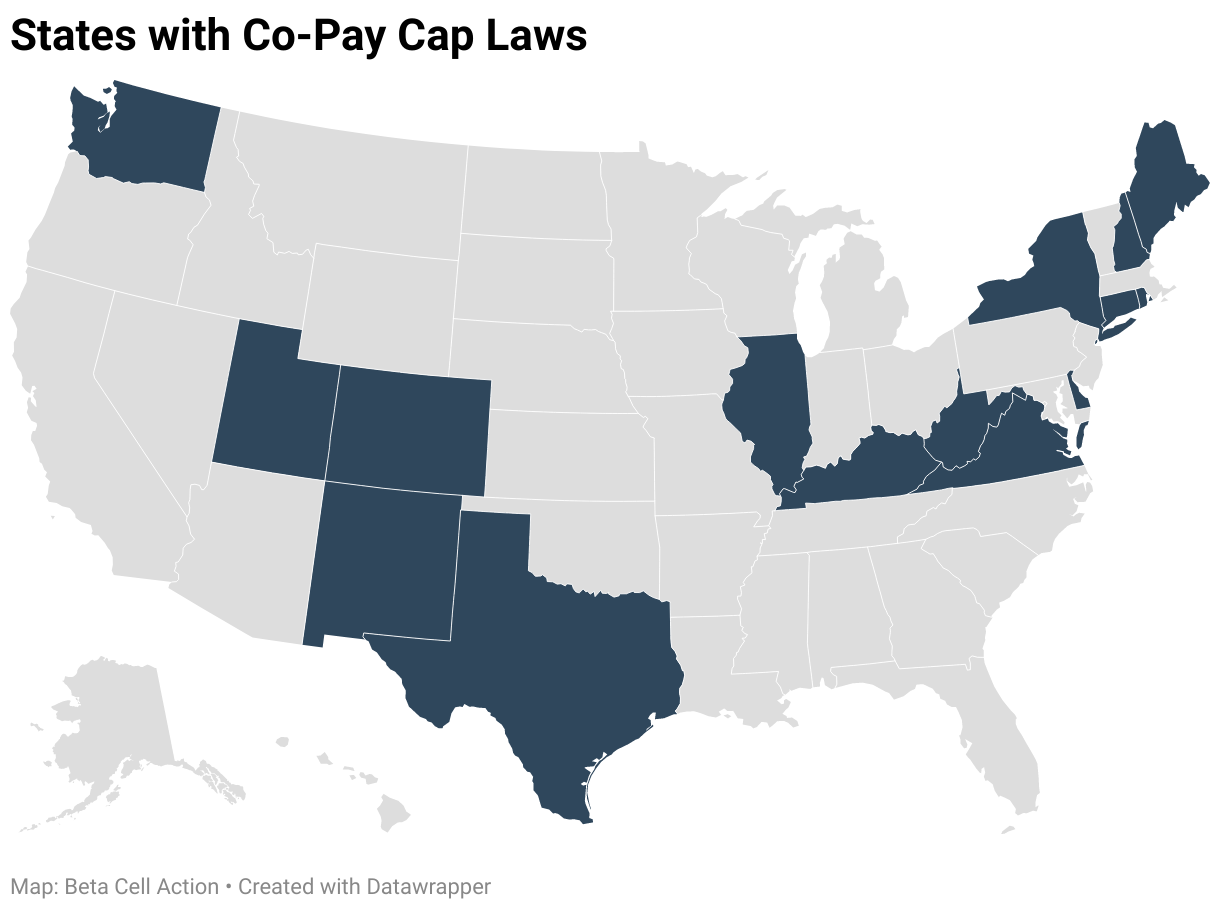
Colorado passed the first insulin co-pay cap in 2019 HB19-1216, capping state regulated insurance co-pay costs at $100 a month per insulin prescribed. Though this created a ripple of excitement in the diabetes community, Colorado residents quickly realized that this bill did not affect all insurance plans.
In a data analysis by Hannah Crabtree, it is estimated that only 29% of Colorado insurance plans are affected by this new legislation. Why such a small percentage? Colorado’s co-pay cap only applies to state regulated insurances. Unfortunately, state co-pay cap legislation only applies to state sponsored plans.
In 2020, the co-pay cap legislation was passed in 6 new states, to a total of 12 states. Hannah Crabtree sought to find out exactly how many people were affected by co-pay caps. Her data analysis revealed that only an estimated 27% of insurance plans nationwide would be affected by a $100 co-pay cap. Even after flaws were exposed in the Colorado bill, states followed this legislative example and left residents in Illinois shocked when their monthly copay caps weren’t capped.
Only an estimated 27% of insurance plans nationwide would be affected by a $100 co-pay cap.
It is clear that the messaging around co-pay caps was confusing and ineffective. That was just the tip of the misinformation iceberg. In recent news, we saw media outlets and legislators exclaiming that individual states had capped the price of insulin. This messaging is very harmful to advocates who now have to discredit legislators and the public, who believe this to be true. Digital advocates have been yelling on social media channels that co-pay caps only regulate state-based insurance plans and not the cost of insulin. Any benefit of co-pay cap legislation will only apply to those with state regulated health insurance, leaving privately insured or not insured out of the equation. Some may argue that this harmful messaging already discredits any benefit from these co-pays caps.
Co-pay cap chaos continued in Montana this last month, when Representative Jessica Karjala hastily introduced HB 222, with hopes to pass a $35/month copay cap. I spoke with Montana #insulin4all advocate, Quinn, to get the scoop.
Quinn, a seasoned advocate in Montana, was shocked to find out about the Montana co-pay cap bill through a long string of second hand accounts. Quinn’s own Representative forwarded an email from one of the supporters and a Diabetes Educator, who then introduced them via email, and then eventually they received a Facebook message from Rep Karjala. “I wouldn’t have even known about this bill if I wasn’t connected to the diabetes educator who sent me an email [describing the bill]… Then I got a text from my childhood diabetes educator (CDE), who connected me to talk to another diabetes educator.” After Quinn got the run around of CDEs, they finally received a Facebook message from the prime sponsor only a few weeks before the bill dropped. If it wasn’t for a myriad of “weird connections,” Quinn may have never even heard about the bill.
Quinn and Rep Karjala’s relationship started when Rep Karjala was just a freshman legislator. Quinn even described their relationship with Rep Karjala as friendly and collegial after they found common ground on Medicaid expansion. Although the energy quickly changed when they discussed this copay cap bill over Facebook Messenger, “When we finally connected over Facebook Messenger, I relayed concerns, I was trying to be diplomatic about things. Starting with ‘I really appreciate you working on this’ while this whole time it felt like she didn’t actually want to listen to what I had to say unless I was wholly in support of the co-pay cap. It appeared she just wanted to move the bill forward with the idea she would help a population of people without actually taking our input into consideration. It felt very disingenuous.” Quinn even goes to describe it as a “Diabetic Savior” complex. After chatting about the bill on Facebook, Quinn expressed some concerns about the limitations of copay caps, sharing that they are supported by Pharmaceutical Research and Manufacturers of America (PhRMA) and that most vulnerable populations, who often don’t have insurance at all, won’t be impacted. Rep. Karjala quickly got “defensive and hostile.” Then, Rep. Karjala turned to Twitter to convey her frustrations.
After an awkward hearing on HB 222, the bill did not pass the House Committee and was tabled.
How does Quinn feel about copay caps overall? “Screen door on a submarine” and “A band-aid on a bullet hole” were two great examples Quinn used to describe co-pay caps. The most glaring issue? These bills leave out the privately insured and the non-insured. Plus, there isn’t a lot of data to show how many people in Montana would be impacted by this bill. “Obviously, we want to help people afford their insulin, but [co-pay caps] are generally not the way to go and are driven by [patient advocacy groups] so they can pat themselves on the back.” Quinn repeatedly called copay caps an “incremental change”, that has the potential to positively impact some people. Quinn shared a couple stories of Montana residents who, on state insurance, pay over $600 a month in co-pays. These folks would have benefited drastically by a $35 dollar cap. If there is a way to help these people, shouldn’t we fight for it?
“Obviously, we want to help people afford their insulin, but [co-pay caps] are generally not the way to go and are driven by [patient advocacy groups] so they can pat themselves on the back.” - Quinn, #insulin4all advocate
But what if there are other incremental changes that could replace the co-pay cap? Quinn shared a couple examples; SB137 “Establishing requirements for transparency in prescription drug costs”, HB345 “Establish Prescription Drug Pay-for-Delay Transparency Act”, and LC2674, which is a revised Alex Smith law being introduced by Montana Rep. Katie Sullivan.
Overall, we can describe Quinn as “not a fan”, of copay caps.
On the other hand, what about the percentage of people who can be affected by co-pay caps? Can co-pay caps work to bridge communities and build relationships? On a call with Legislative Leaders around the country, the co-pay cap dilemma was discussed. In states with conservative leaning politics, co-pay caps may seem like a helpful way to build relationships with legislators and sometimes are the only pieces of legislation that have the potential to be heard.
In conclusion, I believe co-pay caps can be helpful to a small few; if messaging is crystal clear, if representatives work closely with advocates, and if bridges are built that can be used to push more progressive legislation down the road. Co-pay caps can be horrendous and tragic when patients are left out of the conversations, when they are labeled insulin price caps, and when only 27% of patients are affected by them.
Further Reading
Impact of Copay Caps by State (Table), Hannah Crabtree
Launch of U.S. State Legislative Guide for Insulin for All – Guide that includes sections on co-pay caps.